 The Problem IS Blood
The Problem IS Blood ...NOT Blood Vessels!
David C. Korn • Long Life Medical
Long Life Medical Inc • (480) 354-6700
11518 E Apache Trail #115 • Apache Junction, AZ 85220
-
A Preventive Approach to Cardiovascular Disease!
-
In the last few years, healthcare consumers have sparked a renewed interest in preventive medicine in this
country. People are taking more and more responsibility for their own health; this also means they have
assumed an additional responsibility for learning and reading about health matters. A great place to start
one’s health education is with cardiovascular disease--the cause of 44% of deaths in the United States!
Despite disproportionate numbers of heart bypass surgeries in this country which buoy up hospitals’ sagging economic fortunes––all recent indications would suggest that medical doctors may soon spend more time looking at the blood, and less at the blood vessels, in their battle against heart disease and stroke.
Up until currently, top minds in cardiovascular disease have been busily addressing the nation’s number one killer disease as mainly a matter of plugged plumbing. The pipes, they have long maintained, can be patched: reamed out, stretched open more widely, tented up with tiny stakes, or even replaced with long segments of a weaker material. But studies have accumulated showing that roughly half of the people suffering heart attacks do not have the classic, narrowed heart vessels, as in atherosclerotic, calcified plaque, or the typical “plugged plumbing.”
Increasing acceptance of new risk factors for heart attack and stroke are causing experts to take another look. The American Heart Association published a book on “vulnerable plaque” pointing out that maybe doctors should have been looking at the blood and not the blood vessels. At Long Life Medical, we are already attuned to looking predictively at the blood.
- Iron Overload Disease
-
The serum ferritin level test is one simple blood test obtained at a physician’s office that
can save lives by preventing heart attack or cancer. Its use for early detection could also spare
circulation problems, deteriorative brain disease (early memory loss), sexual dysfunction and impotence in
males, occasional infertility in females, cirrhosis, and puzzling night leg cramps in either sex, to name
just a few unpleasant related conditions. However, this test is so neglected in the usual routine medical
assessment, that you often have to ask for it yourself by name, and sometimes even demand it.
This is somewhat surprising, since the Center for Disease Control recommended in 1996 that every primary physician routinely screen his or her patients for Iron Overload Disease, (or IOD)–––a devastating and even deadly illness from iron buildup. The serum ferritin level test is the best screen for IOD. The serum iron blood test–– standard run in most doctors’ offices––is simply not adequate to screen for IOD.
Iron is normally strictly regulated by the small intestine. Too much simply goes out in the stool; and too little is compensated for by its increased absorption through the intestinal wall. But, alas, this perfect system can astray, and at least 1 million Americans have undiagnosed IOD. Some medical studies claim untreated IOD has only 15% survival rate (worse than for many cancers). This disease is entirely preventable, and easily treated, once diagnosed.
The increased iron in the body turns on (catalyzes) the Fenton Reaction, a biochemical reaction in the human body that can lead to increased hydroxyl free radicals. The latter are the most damaging free radicals known. Unbridled, accelerated aging is the result. Many people are written off as cardiac deaths or stroke victims, when in reality, they were really iron overload disease (IOD) persons.
The devastation of IOD is thought to be due to an accelerating effect by the excessive iron on the body’s production of free radicals. These by-products of metabolism (compounds or fragments) are neutralized by antioxidants, like vitamins E , C, as well as enzyme systems in the body. Although the enzyme systems wear out, antioxidant vitamins still help. Free radicals contribute greatly to aging, degenerative diseases, and a general decline in the body’s immune system.
Stubborn elevation of liver enzymes revealed in routine physician testing may also be a sign of undiagnosed IOD, as may cholesterol problems despite scrupulous dieting. The liver (a chief organ for iron storage) has its optimal function diminished by too much iron. Nonalcoholic cirrhosis, and even cancer, can occur from excessive iron. Circulation problems, male impotence, failing memory, acceleration of aging, and sterility in females, can occur from IOD. Too much iron is like throwing gasoline on a free radical fire.
Recommended Tests for a Healthy CardioVascular System Test
Serum Ferritin
Homocysteine
Lp(a)
ISAC (Hemex)
C-Reactive Protein
TOPS
Hair Screening
Risk Factor Identified
Iron excess: increased heart attack and/or stroke
Hereditary: increased heart attack (MI)
Hereditary Lipoprotein-a: Increased MI
Thick blood: low oxygen, clots, (MI)
Inflammation leading to heart attack
Free radical excess, Unhealthy aging
Toxic Metal and Mercury Overload
- Serum Ferritin Levels and IOD Treatment
-
The serum ferritin test is unfortunately not only under-used, but it is often used
incorrectly. The normal level for serum ferritin should not be above 80, according to expert physicians in
the American College for Advancement in Medicine. The Iron Overload Diseases Association in Florida
believes the level should be even lower.
Incidentally, American laboratory reports sent to doctors are notoriously misleading: they list “normal” serum ferritins in the range of from 50 to 300. However, Circulation, a peer-reviewed journal which is a favorite among cardiologists, reported on a Finnish study of just under 1,000 males whose serum ferritins were studied. These patients were tracked for many years to see what happened to them. Patients who had a serum ferritin of 200 or better, a 220% increase in the incidence of heart attack was noted-or 2.2 times the control group. Obviously, laboratory values in the United States are way too high, too permissive for serum ferritin.
If you have a serum ferritin level is around 150, then you should give blood every sixty days at the Red Cross. Excess iron will be controlled in this way.
If your serum ferritin level is over 200, then (as a minimum) you should have a physician write a prescription for a therapeutic phlebotomy at the Red Cross. Your blood will be taken weekly, or more often, depending upon, your hemoglobin tests, done to guide your therapy, along with interval serum ferritin level tests. The objective is to get your serum ferritin numbers down to around 50 as quickly as possible. Maintenance treatments are then done.
The treatment of choice at Long Life Medical for elevated levels is therapeutic phlebotomy (blood letting) and IV EDTA chelation, along with appropriate prescribed free radical quenchers. The bloodletting does not harm patients with IOD. In fact, they often feel better after a treatment. There is no other way to get the iron out other than regular therapeutic phlebotomy.
All people should avoid vitamins with iron and iron supplements, unless advised otherwise by a hematologist.
Elevated Homocysteine Is a Sign of Other Degenerative Diseases Elevated homocysteine can be a sign of a methylation deficiency. Methylation is fundamental to DNA repair. According to a survey in Cardiologia (Apr 1999, 44[4]:341-345) the average American’s homocysteine level is 10 (Highest Risk)!
At Long Life Medical, Inc, this test is routinely gotten on men and women. The complete “heart risk factors” blood test package includes Lp(a), homocysteine, serum ferritin, CRP, TOPS and the ISAC test for thick blood, all of which can be done together at Long Life Medical.
- Homocysteine
-
It has been established that both cardiovascular disease and Alzheimer's disease are linked to the
accumulation of a toxic amino acid called homocysteine. Elevations of homocysteine mean a failure in
the body’s ability to methylate, or detoxify compounds by moving around certain one-carbon fragments.
Methylation is critical to DNA repair. If DNA is not adequately repaired, mutations can occur, leading to
accelerated aging and age-associated disorders, such as cancer, liver dysfunction, memory failure and heart
attack.
Homocysteine was first discovered Kilmer S. McCully, MD –– a Harvard pathologist. The Homocysteine Revolution (1997) chronicles the doctor’s struggles and discoveries. McCully showed not only that those who suffered from this hereditary disorder were at higher risk for heart attack, but also that its successful treatment involved a simple vitamin therapy. For decades, McCully was unrewarded for his work by his colleagues, who ostracized him mercilessly. How could any type of serious heart disease be treated effectively by vitamins?
Shortly after publicizing his work, Dr. McCully had lost his job at Harvard, and ultimately was black-balled at every leading pathology department in the country. Finally, he hired on as a pathologist with the Veteran’s Administration. In the early nineties, McCully was redeemed, and he was paradoxically hailed as a brilliant researcher for his work on homocysteine.
Furthermore, in 1998, it was revealed that elevated homocysteine levels are common in people suffering from Alzheimer’s type of dementia. Earlier research at Tufts University in 1995 documented similar findings linking elevated homocysteine levels and Alzheimer’s disease.
- Reducing Homocysteine Levels
-
Although there remains the question of whether elevated homocysteine levels causes Alzheimer’s or vice
versa, the treatment is basically the same: TMG (trimethylglycine), folic acid, vitamin B6 and vitamin B12
supplementation. Amazingly, as shown by Dr. McCully’s early work, very aggressive vitamin therapy by a
physician knowledgeable in it can reverse this trend. It is extremely important that one does not believe
that they are protected because they are taking folic acid and B vitamins. Studies have shown it is often
not the case! Instead, large doses of Trimethylglycine (TMG) and other “methylators,” with several follow-up
blood tests, may be necessary for complete reversal.
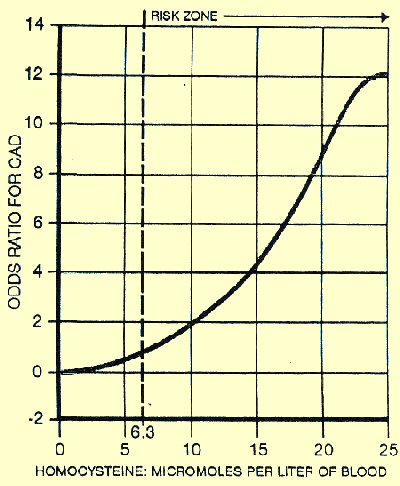
Only by having a homocysteine blood test performed, can one be sure of what his (or her) levels may be. However, once again, it is critical to get a proper interpretation of test results. In addition to being wrong on serum ferritin levels, US labs are also wrong on the ideal range of blood levels for homocysteine. They list 5 to 15 as an acceptable range, but studies have shown problems at values exceeding 6.3. Homocysteine levels above 6.3, are associated with not only increased heart attack risk, but also Alzheimer’s.
If one has an elevated homocysteine level, then he or she should take trimethylglycine, or TMG, 2 or more twice per day with folic acid, B6, and B12. It should be noted that B vitamins are not as effective in lowering homocysteine levels as is TMG, but all are needed. TMG may be acquired at most health food stores, and at the LongLife Medical offices.
- “Thick” Blood
-
The Immune System Activation Of Coagulation (ISAC) Panel of tests (from Hemex Labs) identifies thick blood
which causes a thick sticky material called Soluble Fibrin Monomer (SFM) to be laid down over one’s
capillaries like a thick carpet. The SFM blocks the transfer of oxygen across the capillaries to important
organs.
Heparin shots are used to cleanup SFM deposits and allow oxygen to reach important organs. Increasing the patient’s oxygenation with the use of heparin shots not only protects that patient from a heart attack or a stroke, but it can also make them feel better. The shots are self-administered by the patient, using a tiny insulin needle, just into the fat tissue of the abdomen; they don’t hurt much at all. It feels just like a little sting, but it is well worth the benefits of warding off a heart attack or a stroke! Usually, an ISAC Panel is redrawn after the patient has been on heparin for one month to check for proper heparin levels, reactions, etc. Patients normally do not stay on the shots for more than six months or so.
The ISAC tests also dramatically increases our understanding of disease and the state of our patients health. Scientists have found that even in the absence of an atherosclerotic plaque or blockage in an artery, a sludge-like deposit can rise up in the blood and plug off an important artery. Surprisingly, these sludgelike deposits can contain viruses, bacteria, and fungi. They apparently arise in the area of an inflamed vessel.
The C-Reactive Protein (CRP) has only recently been considered a cardiac risk. The May 2002 issue of Scientific American devoted its feature article to this newly-recognized heart risk. The cover of the magazine featured a human heart, above which bold print declared: A Fire Within. It was subtitled: “Inflammation’s Link to Heart Attacks.” An elevated CRP value says there is inflammation somewhere. Then the search begins.
Agents For Protecting Your Heart Against
New Risk Factors Discussed In This ArticleAgent
Condition Requiring Treatment
TMG (Trimethylglycerine)
Folic Acid
B6 (pyridoxine)
Choline
Elevated Homocysteine indicating a problem in methylation with potential for damage to one’s DNA; heart attack, stroke, memory loss, possibly Alzheimer’s; may need all agents (L)
Niacin, timed release;
Polycosanol
Lp(a) Elevated Cholesterol and triglycerides; Low HDL; take both
Heparin;
SQ “mini-dose”
Hypercoagulable state or ‘thick blood’ (neither aspirin nor coumadin help this condition)
Woboenzyme; FYI;
antibiotics (judiciously used)
Elevated C-Reactive Protein (CRP); Anti-inflammatory, antibiotic actions
MgEDTA IV Chelations
Low TOPS; heavy metal toxicity showing in hair screening; to increase anti-oxidant capacity
Therapeutic Phlebotomy (blood letting)
Iron Overload; Free Radical Excess
Therapeutic Phlebotomy (blood letting)
Small particle LDL; thought to invade the arterial wall; Niacin converts it to large particle LDL
- Lipoprotein (a) ... and the Cholesterol Factor
-
Lipoprotein-a or Lp(a) is a hereditary condition. People who inherit this problem are at much higher risk
for heart attack and stroke. Lp(a) is a special form of LDL, or low density lipoprotein––bad cholesterol.
(Remember that HDL stands for Healthy cholesterol; the “H” stands for “Healthy.” All the rest is
“bad” cholesterol, i.e.; LDL and VLDL.)
There have been many treatment regimens attempted over the years for Lp(a), but the best routine must include Niacin, or B2, since it has been proven to lower Lp(a). Many people avoid Niacin because of the well-known “Niacin flush,” which is associated with heat, redness, and itching. However, the timed-release form of Niacin has little, if any “flushing” (hot, red, itchy) effect. Timed-release Niacin also changes small particle LDL into large particle LDL. Small particle LDL is believed to infiltrate the arterial wall (because of its tiny size) and set off an injury chain of events that culminates in an atheroma––a “tumor” or calcified cholesterol growth which blocks the channel within the artery.
Elevated total cholesterol with low HDL is still a serious risk factor, as are high triglycerides. There are good natural products which will help elevate HDL and lower LDL and VLDL, while lowering triglycerides. The newest such product is polycosanol. This is often prescribed along with timed-release Niacin (ie. Enduracin).
- Your Personal Plan ...
-
At the bottom of the column is a table summarizing the items discussed in this article. Dosages are not listed
since these vary widely from person to person. It is extremely important to realize that one size does NOT
fit all, and each person needs to work with his (or her) doctor on a comprehensive health program.
Anyone wishing to identify their cardiovascular risk factors should call the Long Life office at (480) 354-6700 and schedule a face-to-face meeting with the doctor and to have the “heart risk factors” blood test package drawn. It could be the best investment you ever make!__DK